Table of Contents[Hide][Show]
If you’ve been told you have prediabetes, you may have heard words like “manage it” or “prevent diabetes.” But what if the goal wasn’t just prevention or management—but remission?
In this episode, Dr. Jedha explores what “prediabetes remission” really means, and why it should be your top health priority with prediabetes.
LISTEN TO THE PODCAST
CHAPTERS
3:09 What is prediabetes remission?
5:40 Should prediabetes remission be your goal?
8:04 Normal glucose regulation cuts risk of type 2 diabetes
13:01 Normal glucose to prediabetes explained
15:20 Two key targets for prediabetes remission
17:45 Insulin sensitivity and visceral fat impact
Definition of Normal Glucose, Prediabetes & Type 2 Diabetes
Current diagnostic criteria, according to American Diabetes Association guidelines.
| Measure | Normal | Prediabetes | T2Diabetes |
|---|---|---|---|
| Fasting Blood Glucose (FBG) | < 100 mg/dL (< 5.6 mmol/L) | 100–125 mg/dL (5.6–6.9 mmol/L) | ≥ 126 mg/dL (≥ 7.0 mmol/L) |
| Oral Glucose Tolerance Test (OGTT) (2hrPG) | < 140 mg/dL (< 7.8 mmol/L) | 140–199 mg/dL (7.8–11.0 mmol/L) | ≥ 200 mg/dL (≥ 11.1 mmol/L) |
| HbA1c | < 5.7% (< 39 mmol/mol) | 5.7–6.4% (39-47 mmol/mol) | ≥ 6.5% (≥48 mmol/mol) |
What Is Prediabetes Remission?
You’re diagnosed with prediabetes when your blood glucose levels are elevated, but not high enough to meet the threshold for type 2 diabetes.
It’s often seen as an in-between stage, but here’s the powerful truth: you can restore normal glucose regulation. That’s what remission means. Not just halting the progression of prediabetes to type 2 diabetes, but returning your blood sugar to normal, healthy levels.
According to research, prediabetes remission is defined as:
- Fasting glucose below 100 mg/dL (5.6 mmol/L)
- A1c below 5.7% (39 mmol/mol)
- 2-hour glucose tolerance test below 140 mg/dL (7.8 mmol/L)
- All achieved without glucose-lowering medications, even Metformin, for at least 3 months
This definition brings clarity—and hope. Because aiming for remission isn’t just wishful thinking, it’s entirely realistic.
In fact, our members in the Prediabetes Reset Program are doing just that, often in as little as 3 to 6 months.

As a result of the information and encouragement I received from Dr. Jedha and the DMP program, I went from an A1c of 6.3 in February to an A1c of 5.8 in April — another month later it went down to 5.7!
The program works! I am so grateful for this program in helping me regain a sense of empowerment.
~Ann

Last week I went in for my yearly physical and my A1c was 5.5!
The doctor had told me that if I could keep my A1c under 5.7 for a year he would take me off metformin.
So… I’m off metformin and you could say that I’m not prediabetic anymore!
~Cheryl
Why Prediabetes Remission Matters
Most health guidelines focus on preventing type 2 diabetes, often emphasizing weight loss and exercise. But they rarely mention remission, despite the fact that research clearly shows it’s achievable and protective.
Let’s break this down:
- In the Diabetes Prevention Program, about 50% of participants with prediabetes achieved normal glucose regulation at some point.
- Those who did had a 56% lower risk of progressing to type 2 diabetes.
- Even achieving normal glucose regulation just once cut the risk by 47%.
- Achieving it three times? That lowered the risk by 67%.
That’s powerful. Even temporary periods of normal blood sugar can make a significant difference.
But it’s not just about diabetes prevention. Even in the prediabetic range, you’re already at higher risk of heart disease, stroke, nerve damage, eye problems, and kidney issues. Restoring normal glucose helps prevent these complications too.

Two Key Drivers of Prediabetes, and Remission
You might be wondering, what actually causes blood sugar to rise into prediabetes in the first place?
According to research there are quite a number of factors:
| Demographic and Adiposity measures | Plasma lipid and amino acid levels |
| • Older age | • Higher triglycerides |
| • Male sex | • Higher LDL/Lower HDL cholesterol |
| • Higher body mass index | • Higher asparagine/aspartic acid |
| • Higher waist circumference | • Higher glutamine/glutamic acid |
| • Higher total and abdominal fat | • Lower histidine |
| Glucoregulatory measures | Miscellaneous measures |
| • Upper-normal FPG and 2hrPG | • Higher blood pressure |
| • Lower insulin sensitivity | • Lower adiponectin |
| • Impaired insulin secretion | • Higher hematocrit |
| • Lower disposition index | • Higher alanine aminotransferase |
But, research points to two key culprits:
- Reduced insulin sensitivity (or insulin resistance)
- Increased visceral fat (deep belly fat around your organs)
Let’s explore why these matter.
1. Insulin Sensitivity
Insulin is the hormone that helps move glucose into your cells for energy. When your cells respond well to insulin, blood sugar stays balanced.
But in prediabetes, cells become resistant. Your body makes more insulin, but it doesn’t work as effectively. Over time, this leads to rising blood glucose levels.
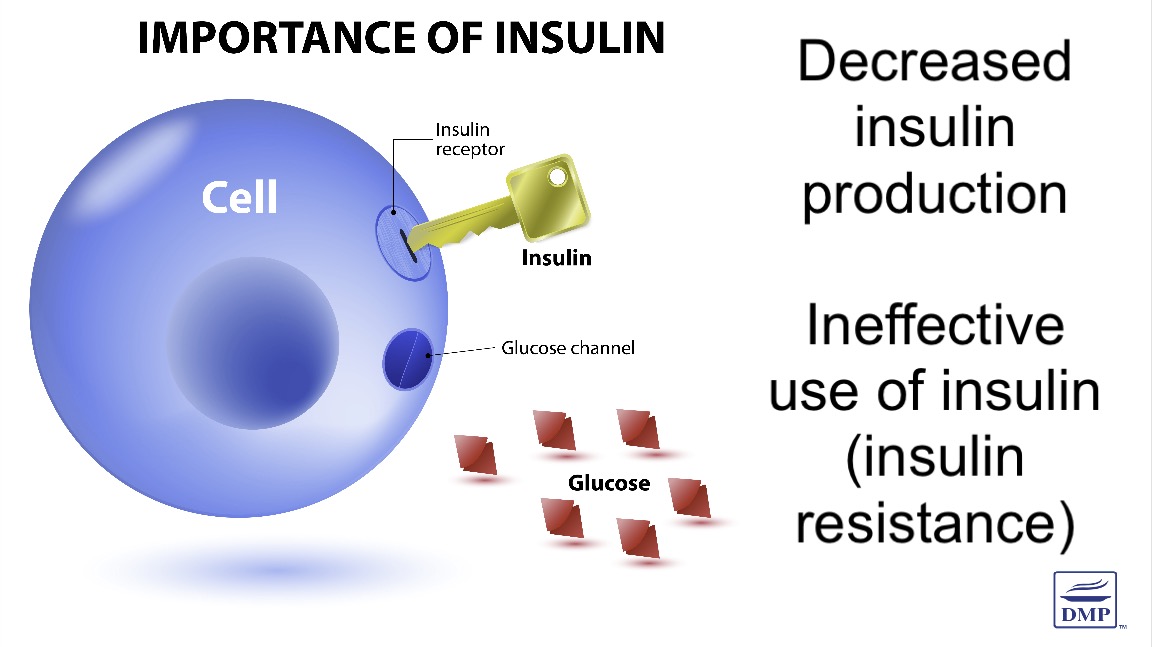
Improving insulin sensitivity means your body can respond better to insulin again, and glucose can be used more efficiently.
2. Visceral Fat
This is fat that surrounds your liver, pancreas, and other internal organs. Unlike the fat you can pinch, visceral fat is biologically active, it releases inflammatory molecules and hormones that disrupt your metabolism.
Visceral fat directly contributes to insulin resistance, raises cholesterol and triglycerides, and can even affect your pancreas, worsening insulin secretion. Reducing this fat has been shown to rapidly improve blood sugar regulation.
What Can You Do Next?
While this episode and info focuses on understanding why remission should be your goal, let’s leave you with a few practical next steps:
- Know your numbers. Use the American guidelines as your goalposts:
- Fasting glucose: <100 mg/dL (5.6 mmol/L)
- A1c: <5.7% (39 mmol/mol)
- 2-hour post-meal glucose: <140 mg/dL (7.8 mmol/L)
- Focus on root causes. Instead of just trying to lose weight, target the root drivers—improve insulin sensitivity and reduce visceral fat. These are more powerful predictors of remission than weight loss alone.
- Be proactive. Don’t wait for guidelines to catch up. Medical care still tends to “manage” prediabetes and prescribe Metformin, rather than aim for remission. But you don’t have to settle for that. With the right strategies, you can restore normal glucose regulation.
One Final Thought
You don’t have to wait until you “have diabetes” to take action. Prediabetes is a window of opportunity. A chance to pause the progression and reverse the course.
Even small improvements in blood sugar can dramatically change your risk trajectory and protect you from serious complications.
So yes—prediabetes remission is possible, and it should absolutely be your goal.
👉 Ready to take action?
Join the Prediabetes Reset Program and get the tools and support you need to achieve remission in 3–6 months. You can do this, and we’ll show you exactly how.
Transcript
Click Here To View
Dr Jedha, Host
Hello there, Dr Jedha here and thanks for joining me for episode 87. I came across a paper recently on a topic that hasn’t really been discussed in the academic literature—prediabetes remission. It wasn’t until 2021 that all the diabetes organizations across the globe published position statements acknowledging type 2 diabetes remission, as a thing, because they couldn’t ignore the surmounting research. But remission of prediabetes, this is not something that has been discussed in the literature, so this paper caught my eye.
People, including researchers, just haven’t thought of prediabetes being put into “remission.” Preventing type 2 diabetes, yes. Managing prediabetes, yes. But prediabetes remission, no. Certainly, we’ve been helping our prediabetes members achieve remission for over a decade—so of course we know it’s more than possible. But it’s interesting that this has now emerged into the research field so I expect we’ll start seeing more and more research appear in this area.
One of the things I liked about this paper, was that the authors highlighted that remission of prediabetes should be considered in guidelines and recommendations for the delay and prevention of T2D, and I absolutely agree. Currently it’s not, and we’ll get to that shortly.
Before we move on I wanted to mention this episode is part 1 of a 2-part prediabetes remission series. We’ll cover what prediabetes remission actually means and why it’s so important for you to have this as your goal. In part two, we’ll cover more of the practical ins and outs and some strategies to achieve prediabetes remission. If you want to be notified by email when new episodes are available, and receive additional tips to help you improve your prediabetes, go subscribe to our weekly enews at type2diabetestalk.com/news
03:09
Okay, let’s start at the beginning by discussing what prediabetes remission means. You get diagnosed with prediabetes when your blood glucose levels are higher than normal but not high enough to be diagnosed with type 2 diabetes. Glucose becomes dysregulated over a spectrum, a period of time, often over years, so we can think of prediabetes as an intermediate stage between normal glucose regulation and type 2 diabetes. When we discuss prediabetes remission, we’re talking about restoring normal glucose regulation.
We spoke about prediabetes glucose goals in episode 72, but let’s just recap the numbers so we can establish what normal glucose regulation is.
Depending where you live in the world, the numbers can vary, so for the sake of this episode on remission, let’s use the American guidelines to establish normal glucose regulation because these are lower than most places and a better long term target to aim for. A normal fasting glucose is below 100 mg/dL or below 5.6 mmol/L, a normal A1c level is below 5.7% or below 39 mmol/mol. A normal postprandial blood glucose level is below 140 or below 7.8.
When we look at the scientific definition for prediabetes remission, it is basically those numbers I just stated, and I quote from this new research study: “prediabetes remission is defined by normal fasting blood glucose (<100 mg/dl, <5.6 mmol/l), normal glucose tolerance (2-h plasma glucose level <140 mg/dl, <7.8 mmol/l), and HbA1c <39 mmol/mol (<5.7%), without glucose-lowering medication for at least 3 months.”
05:40
Absolutely your goal with prediabetes should be prediabetes remission, restoring normal glucose regulation. As I said, this is what we help our members do, but over the years, we haven’t called it ‘remission’. We often just position it as getting back to normal or reversing prediabetes. Of course it seems obvious that this should be the goal for everyone with prediabetes. But it’s actually not the primary goal in current medical care guidelines. As we spoke about in episode 69, prediabetes has become an overmedicalized health condition where medication is often prescribed but not necessary.
Overall, when we look at the medical care guidelines, we currently don’t have a section dedicated to prediabetes treatment. That’s surprising given the rates of prediabetes across the globe. Currently, the medical care guidelines put an emphasis on preventing type 2 diabetes, with a whole chapter about that. But the focus is on weight loss and physical activity, and overall, when discussing prediabetes, they refer to “management” of prediabetes.
It’s assumed among many health professionals that most people with prediabetes will go on to get diabetes, so it’s great that this conversation about prediabetes remission has started in the academic literature, because certainly it was once thought that type 2 diabetes was a progressive disease that was destined to get worse – now we know that’s not true it can be reversed and put into remission. Likewise, thinking that prediabetes is destined to get worse is clearly not the forward-way of thinking, and we know it is certainly not true by any means. Prediabetes is absolutely reversible and can be put into remission. Unfortunately, as is often the case, it’s probably going to take years before we see this reflected in the medical care guidelines, which is why you always need to be proactive with your own health.
So, prediabetes remission, it’s not something that’s really been studied, it hasn’t been a primary outcome or objective of previous studies.
08:04
When we look at previous lifestyle intervention studies, like the Diabetes Prevention Program and others, prediabetes remission occurred in around 50% of participants. These studies have shown that with lifestyle intervention, your risk of getting type 2 diabetes over a 7-30 year period is reduced by 27-43%. Certainly that’s quite a lot. But, something to note, and this is important, is that these interventions did not have a goal of prediabetes remission, but T2Diabetes ‘prevention.’ These studies did not specifically aim for people to achieve normal glucose regulation (NGR). If they had, the outcomes would likely have been a lot better.
Currently there are few studies that have pre-specified regression of prediabetes as the primary outcome so we don’t have a lot of long term data on this but in the Diabetes Prevention Program Outcome Study, participants with prediabetes who achieved NGR at least once during long-term follow-up had a 56% lower risk of getting T2D compared with those who never achieved NGR. In fact, the number of times a participant achieved NGR was shown to have a direct association with the risk reduction in progressing to T2D: 47% reduced risk when NGR was achieved just once, 61% reduced risk when NGR was achieved twice, and 67% reduced risk when NGR was achieved three times.” This is incredibly powerful, as it indicates that if you achieve and maintain normal glucose levels, your risk of T2D is dramatically reduced, if not mitigated altogether. The other thing this data indicates is that even if you have transient periods of maintaining NGR in prediabetes, this also decreases your risk of developing T2D. In another study, participants who returned to NGR had a 73% decreased risk of getting T2D within 3 years of the study. While we don’t have long term data on this, without a doubt, having NGR as your goal, dramatically reduces your risk of type 2 diabetes, if not eliminating your risk altogether.
The benefits of aiming for normal glucose regulation go beyond developing type 2 diabetes. By aiming for normal glucose regulation, you dramatically decrease your risk of microvascular complications like retinopathy, neuropathy, and nephropathy; and macrovascular complications like heart attack and stroke. Why? Because these complications occur due to higher than normal blood sugar exposure over time. If your blood glucose is normal, you’re not going to develop these complications.
And just going back to those medical care guidelines again, they focus a lot on weight loss in prediabetes and for diabetes prevention. But research shows us that while weight loss is important, weight loss without reversion to NGR is not associated with the same risk reduction as weight loss in combination with reversing to NGR, so to emphasize again, your goal with prediabetes is remission, to achieve normal glucose regulation.
13:01
Let’s explore how a person goes from normal glucose regulation to prediabetes, because this gives us clues on what we need to do to reverse this in the opposite direction, to prediabetes remission.
Studies have looked into the factors that predict the transition from a state of NGR to prediabetes. First I’ll go through all the factors mentioned in the literature, then I’ll come back and focus on two particular factors.
Factors include weight gain, higher BMI and waist circumference, insulin resistance, pancreatic beta-cell dysfunction with impaired insulin secretion, increased production of inflammatory molecules, dysfunctional incretin hormone response, altered liver glucose production, changes in cholesterol such as high triglycerides, high low-density lipoprotein cholesterol and lower HDL cholesterol and adiponectin levels, high blood pressure, FPG and 2hrPG at the upper end of the normal range, older age, male gender, changes in amino acid levels, and various others things—we’ll leave a chart of these in the show notes.
So a lot of these factors are interesting right, because if you’ve listened to other podcasts episodes, you’ve heard me speak of how prediabetes is a condition of altered metabolism and how factors such as cholesterol and blood pressure are often connected to prediabetes, and these various studies also highlight this. Although these conditions are often treated as isolated conditions, they are often a cluster and why this is interesting, is that these factors in isolation are potential indicators that prediabetes or rather dysregulation of blood glucose could be imminent. Doctors could be doing more synergistic assessment, rather than just looking at things in isolation.
15:20
Let’s come back to the two particular factors that seem to be major drivers in prediabetes remission. Number one: improving insulin sensitivity and reducing insulin resistance and number two: reducing visceral fat.
Overall, the evidence suggests that people who progress from NGR to prediabetes have lower insulin sensitivity compared to people who don’t progress; and also a steeper decrease of insulin sensitivity over the years.
Insulin sensitivity refers to how effectively the body’s cells respond to insulin, a hormone that helps regulate blood sugar levels. Higher insulin sensitivity allows cells to use glucose more efficiently, whereas insulin resistance is where the body’s cells do not respond properly to insulin, the body doesn’t use insulin efficiently and this leads to higher blood glucose levels. We know that insulin resistance is one of the key causes and underlying factors in both prediabetes and type 2 diabetes.
Visceral adipose tissue, or visceral fat, is a type of body fat that is stored deep within the abdominal cavity, surrounding vital organs like the liver and intestines. Think of this as deep belly fat, as it is most typically around the midsection. Most of us think this fat just sits there, but visceral fat is a hormonally active tissue, it releases different hormones and inflammatory molecules.
If we can focus our attention on these two factors – insulin sensitivity and visceral fat, we’ve got a powerful combination for prediabetes remission.
Before we chat about how these are connected to blood glucose regulation, let’s hear a testimonial from one of our members.
7:45
When we think about insulin sensitivity and visceral fat, understanding their impact on your blood glucose regulation becomes critical. These two factors don’t work independently—they profoundly influence each other, and can create a vicious cycle.
Remember, insulin sensitivity is your body’s ability to efficiently utilize insulin, allowing glucose to be effectively absorbed by your cells, which in turn helps maintain stable blood sugar levels. When your body is sensitive to insulin, your pancreas doesn’t have to work overtime producing excessive amounts of insulin, and your cells efficiently absorb glucose, keeping your blood sugar in check.
On the flip side, visceral fat dramatically reduces your insulin sensitivity. Think of visceral fat as not just passive storage but rather an active endocrine organ. It releases hormones and substances called cytokines and other inflammatory molecules, which directly interfere with your cells’ ability to respond effectively to insulin. More visceral fat means more inflammation, greater insulin resistance, and higher blood glucose levels. Free fatty acids (FFA) from visceral adipose tissue in the body can drain directly to the liver, contributing to deposits of fat in the liver and contributing to increases in cholesterol and triglyceride production, and very low density lipoprotein. And these FFAs can also enter circulation, affecting other organs such as the pancreas, which can affect beta-cell function and insulin secretion – so again, we see all these mechanisms throughout our miraculous body are connected in very intricate ways.
Research shows us clearly that reducing visceral fat significantly improves insulin sensitivity. This means your body starts responding better to insulin, inflammation reduces, and blood sugar regulation improves dramatically, and it rebalances all these other processes occurring in your body. In fact, even modest reductions in visceral fat have powerful impacts, rapidly improving your blood glucose control and reducing your risk of type 2 diabetes.
So where does that leave us?
Well, preventing a type 2 diabetes diagnosis is clearly a worthwhile pursuit. But remember, another very important reason you want to get your prediabetes back to a normal glucose state is that even in prediabetes you’re at risk of developing microvascular complications and macrovascular complications. These are serious things that you can prevent, so the benefits of getting your blood glucose back to normal cannot be overemphasized. Prediabetes gives you the opportunity to make significant changes to better your health.
Remission is your goal, restoring normal glucose regulation. Restoring balance and harmony to your body.
A quick recap on those goal numbers, based on American guidelines: A normal fasting glucose is below 99 mg/dL or 5.6 mmol/L. Normal postprandial levels are below 139 or 7.8. A normal A1c level is under 5.7% or 39.
The process of losing blood sugar control happens on a spectrum, so the sooner you can take action after a diagnosis, the sooner you can restore normal glucose regulation and rebalance your metabolism back to normal.
Of course, if you need help to do that, join the Prediabetes Reset Program—our members are restoring normal glucose regulation within 3-6 months so let us help make the whole process easier for you.
And I know I’ve left you hanging a bit here, because you’re no doubt wondering HOW you can target insulin sensitivity and visceral fat and that’s exactly what we’ll cover in Prediabetes Remission: Part 2, available in another episode very soon. For part 2 in this series, we will explore evidence-based strategies that directly target insulin sensitivity and visceral fat. You won’t want to miss that so if you want to be notified by email when episodes are available, join our enews at type2diabetestalk.com/news. And if you’ve found this episode interesting, please share it with a friend, family member or colleague.
That’s all for now.
Dr Jedha, over and out.
Prediabetes Food List: Grab Your Free Copy
Foods to eat and avoid, plus, 2 day sample menu
Subscribe to Type 2 Diabetes Talk on: Apple | Spotify | Amazon Music | Audible | YouTube | Podcast Index | Player FM | and more…
Leave a Reply