If you’ve been diagnosed with type 2 diabetes or prediabetes, chances are you were given dietary advice based on official guidelines. You may have been told to eat whole grains, balance your meals, watch portions, limit fat, and individualize your food choices.
On the surface, that sounds sensible. Many of us have heard this type of thing our whole lives.
But if you’ve followed that advice and still struggle with high blood sugar, rising A1c, weight gain, or increasing medications, there’s a reason. The problem isn’t your effort. The problem is that the nutrition guidance itself lacks clarity, structure, and a true understanding of what’s going on in diabetes metabolism.
Each year, the American Diabetes Association releases its updated Standards of Care. The document is hundreds of pages long and packed with scientific references. Yet when you get to the nutrition section, the same issues remain. If you live in Canada, UK, Australia or elsewhere, the issues are the same.
The guidelines continue to say there is no ideal percentage of carbohydrates, protein, and fat. They emphasize individualization and state that many eating patterns can be appropriate.
While that may sound flexible and patient centered, in reality it leaves people with diabetes without the specific guidance they actually need.

Vague Advice Doesn’t Lower Blood Sugar
People with type 2 diabetes don’t struggle because they lack options. They struggle because they lack direction.
The ADA guidelines offer no clear carbohydrate targets. There’s no practical guidance on how much carbohydrate is too much for blood sugar control.
There are no meaningful protein intake recommendations, despite strong evidence showing protein plays a central role in insulin sensitivity, muscle maintenance, appetite regulation, and glucose control.
Instead, people are told to balance meals, watch portions, choose whole grains, limit saturated fat, and personalize their diet.
But none of this explains why blood sugar rises after meals, what actually drives A1c higher, or how to consistently improve diabetes metabolism.
Without structure, people are left guessing. Scrambling. Following bad advice.
And when results don’t come, many people quietly assume they’re failing.
The Missing Piece, Carbohydrate Quantity
One of the biggest problems with the ADA nutrition guidance is its reluctance to directly address carbohydrate quantity.
Decades of physiology and clinical research show that carbohydrates are the primary driver of post meal blood sugar spikes. They are also the main contributor to elevated HbA1c levels.
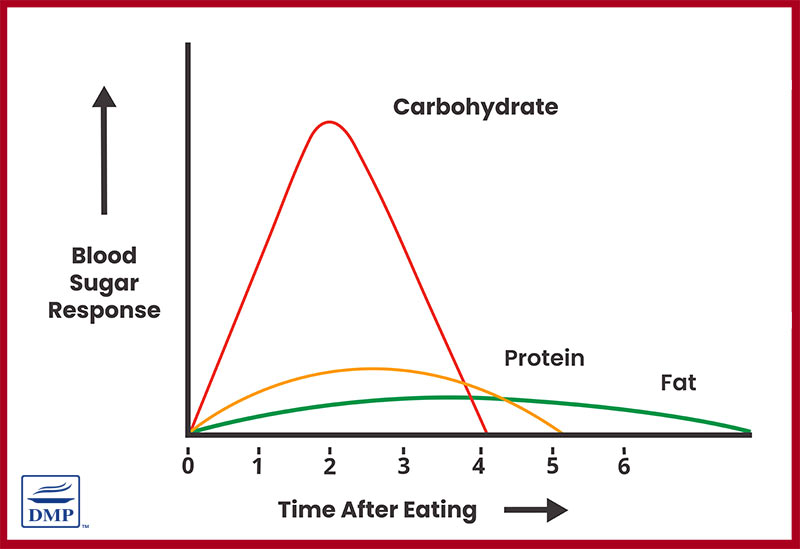
Way back in the 2005 ADA guidelines, they stated that carbohydrate quantity was critical to diabetes management. Yet in 2026, the ADA continues to avoid setting carbohydrate ranges or thresholds?!
That doesn’t make sense and it’s not evidence-based either.
Instead of saying clearly that reducing carbohydrate intake improves glycemic control, the guidelines frame all macronutrient distributions as equally acceptable.
This creates confusion. And, based on science, it’s inaccurate.
A person could follow the guidelines while eating a high carbohydrate diet built around whole grains, fruit, and low fat foods, yet still experience large glucose spikes and worsening insulin resistance.
Another person might reduce carbohydrates significantly and see rapid improvements in blood sugar and A1c.
Both approaches are technically considered “acceptable” under the ADA guidelines, even though the outcomes are often dramatically different. There’s plenty of science to tell us what the recommendations should be.
The lack of specificity in the ADA guidelines is not helpful in a condition where glucose regulation is the central issue.
The problem: most people eat too many carbohydrate foods and the wrong types so they struggle to achieve and maintain good blood sugar levels.
Protein Is Still Treated as an Afterthought
Another major gap in the ADA guidelines is protein.
Despite strong evidence showing that adequate protein intake improves metabolic health, supports lean muscle mass, and helps stabilize blood sugar, the guidelines avoid providing clear protein targets.
Instead, they focus largely on protein sources, often discouraging red meat and emphasizing plant-based proteins, without solid evidence that this improves outcomes in diabetes.
The problem isn’t plant protein itself. The problem is avoiding clear guidance on how much protein the body actually needs. And providing guidelines that aren’t backed by solid evidence.
For many people with insulin resistance, under-eating protein contributes to muscle loss, slower metabolism, increased hunger, and poorer glucose control.
Without addressing protein intake directly, a major tool for improving metabolic health is being overlooked.
The problem: most people don’t eat enough protein and need to eat more of it — all types, including nutritious meats.

Outdated Fat Fears Still Linger
Although research over the past decade has consistently shown that whole food sources of fat, including full fat dairy and natural animal fats, do not worsen cardiometabolic health in the way once believed, the ADA guidelines continue to favor low fat or fat free options.
This stems from outdated thinking that saturated fat automatically increases heart disease risk.
For people with diabetes, replacing fat with carbohydrates often worsens blood sugar control and insulin resistance.
Yet the guidelines still subtly promote lower fat eating patterns, even when evidence suggests food quality and carbohydrate load matter far more.
KEY POINT: There is zero evidence that saturated fat worsens heart disease or diabetes.
Individualization Without a Framework
One of the most repeated words in ADA nutrition guidance is “individualization.”
In theory, tailoring nutrition to the person sounds ideal. In practice however, without a clear framework, it becomes meaningless.
True individualization should still be built on physiological principles. Carbohydrate raises blood sugar, protein supports metabolism and insulin sensitivity, ultra processed foods worsen metabolic health—plenty of evidence to support that.
Instead, the guidelines present a wide range of eating styles as equally valid, without explaining which ones are most effective for blood sugar control. Science does not put all eating styles equally!
This puts both patients and healthcare providers in a difficult position.
Doctors and dietitians often want to help, but without clear guidance, they default to broad, generic advice that rarely produces strong results.
Why This Matters in Real Life
The consequences of vague nutrition guidance are very real.
Many people spend years trying to manage diabetes through “healthy eating” as defined by the guidelines, only to watch their numbers slowly worsen. Medications are added. Doses increase. Complications become a concern.
All the while, they may never be told that reducing carbohydrate intake, prioritizing protein, and focusing on whole foods could dramatically improve their blood sugar.
This isn’t about extreme diets. It’s about aligning nutrition advice with how the body actually works.
When people finally receive clear, structured guidance, the results are often profound. Blood sugar drops. A1c improves. Weight becomes easier to manage. Medications can often be reduced under medical supervision.
That clarity is what’s been missing. And this shouldn’t be the case when there is plenty of evidence to support better, clearer guidelines.
One Practical Step That Makes a Difference
If there’s one change that consistently helps people improve blood sugar control, it’s this.
Prioritize protein at every meal and reduce refined and high carbohydrate foods.

Adequate protein helps stabilize glucose levels, improves insulin sensitivity, supports muscle mass, and reduces cravings that drive overeating.
Combined with lowering carbohydrate intake, it creates a metabolic environment where blood sugar can finally come down.
Conclusion
The ADA guidelines have evolved in many areas of diabetes care, but when it comes to nutrition, they continue to avoid providing the clear, actionable guidance people need.
By failing to directly address carbohydrate quantity, by under emphasizing protein, and by holding onto outdated fat fears, the guidelines leave millions of people confused and stuck.
Progress is happening in broader nutrition policy, but diabetes specific guidance still lags behind the science—way behind!
Until that gap closes, real improvement will continue to come not from vague outdated advice, but from structured, evidence based approaches that reflect how metabolism truly works.
And when clarity replaces confusion, better health finally becomes achievable. That’s exactly how we help our members!
rebecca coleman
I am 64 years old, female. I have been reading your website since Oct 2025. I was diagnosed prediabetic in Oct 2025, I not on any medications for diabetics. I have followed the advice on your website (low carb, no bread, rice, potatoes at all, low fat meats 5 days a week, 2 days a week saturated fat meat (beef), & green vegis) diet since that time. My A1C in Oct was 6.4 it dropped to 5.8 by Jan 29 2026. my total cholesterol went from 219 to 117 in that same time. LDL cholesterol was 112 in Oct now 115. I’ve lost 27 pounds, I started out at 155 in Oct, now I’m 127. I do moderate exercise every day, I feed goats, rabbits, chickens twice a day every day. I eat the rabbits and eggs and some of the old hens. My doctor wanted to put me on Metformin in Oct, I said let’s try diet/lifestyle changes first. They are happy with my results at the end of January 2026 said I don’t need to come back for further testing for 1 year as long as I keep up the same diet changes. My father was diabetic on Metformin for over 10 years he died in 2011 at 82 of pancreatic cancer. I’m just trying to get some reassurance on this diet and lifestyle changes. I can’t afford to join the website (feed costs have risen the past 5, 6 years).
will my A1C continue to drop to below prediabetic ranges?
Is there a way to get my LDL cholesterol down also?
will I continue to lose weight and is it normal to lose about 1 pound per week?
any more info would be helpful, if possible, thank you Rebecca Coleman
Dr Jedha
Hi Rebecca, it sounds like things are going well for you and your numbers have improved a lot in a short time so keep doing what you are doing and your A1c should continue to improve, along with weight and other numbers. I would recommend this podcast on understanding cholesterol. The important thing is patience. Your body didn’t get to prediabetes overnight or within 3 months. Improving health takes time and a consistent proactive approach, which is exactly what it sounds like you’re doing.